World Health Organization 2018 guidelines recommend Sofosbuvir (SOF)/Daclatasvir (DCV) as a pangenotypic regimen for the treatment of adults with chronic HCV infection. SOF/DAC is widely available as low-cost generic formulation in low and middle-income countries (LMICs). Recent studies in adolescents (?12 to <18) using SOF/DCV 400/60 mg once-daily (OD) adult dose reported excellent efficacy and safety. DCV pharmacokinetic (PK) data in younger children are lacking. Within the framework of the Global Accelerator for Pediatric Formulations (GAPf), we performed a population PK analysis using data from adolescents to predict DCV exposure in children <35 kg to determine the lowest body weight children could be treated with the available DCV formulations (60 and 30 mg).
Data from HCV-infected adolescents receiving SOF/DCV (400/60 mg, OD) who participated in a PK study in Egypt were used for PK model development. Intensive PK sampling was performed pre-dose, then 0.5, 1.0, 1.5, 2, 4, 8, 12, and 24 hrs post-dose. PK parameters were estimated using a population approach (NONMEM VII). Monte Carlo simulations were run for virtual children between 10 to <35 kg receiving 60 mg or 30 mg OD and DCV exposures (AUC0-24) were compared with the expected adults range (6.15 to 20.63 µg.hr/mL).
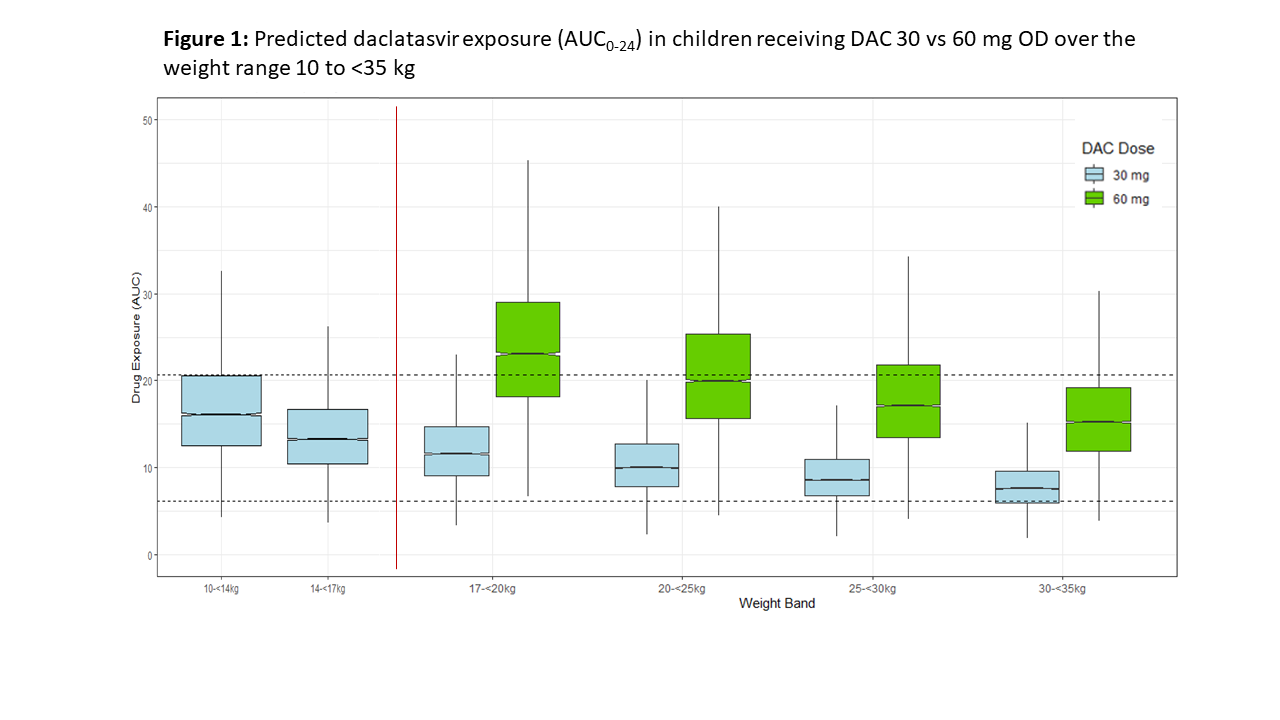
Seventeen HCV-infected adolescents (13 males) provided 151 DCV concentrations. Median (range) age was 14 (11-18) years and weight 50 (32-63) kg. DCV plasma concentrations were best described by a 1-compartment model with transit absorption compartments. Body weight (allometrically scaled) and albumin influenced DCV PK parameters. DCV oral clearance and volume of distribution were 7.05 L/hr/70kg and 95.8 L/70kg. In adolescents using 60 mg DCV OD, mean (SD) DCV AUC0-24, Cmax, and Clast were 12,004 (4,916) ng.hr/mL, 1,182 (393) ng/mL and 194 (168) ng/mL, respectively; while predicted to be 9,808 (3,949) ng.hr/mL, 1,039 (316) ng/mL and 148 (129) ng/mL in children 17 to <35 kg receiving 30 mg OD. Simulations showed that the proportion of children with DCV exposures above expected range rapidly increased for children <30 kg using 60 mg OD; and similarly for children 10-14 kg using 30 mg (Fig 1).
DCV 30 mg OD is expected to provide exposures comparable to adult values in children 14-35 kg. Our results suggest that children could be treated using currently available low-cost DCV formulations together with approved doses of pediatric SOF formulations, thus expanding access to HCV treatment.