Responding quickly to potential HIV outbreaks, a pillar of the U.S. Ending the HIV Epidemic (EHE) initiative, requires timely HIV case and sequence reporting. Expediting reporting of case reports, needed to detect clusters of increased diagnoses, and HIV sequence data, needed to detect molecular clusters, will be a key activity in EHE-funded programs. We describe the baseline timeliness of HIV case and sequence reporting to health departments overall and by geographic characteristics.
Using data reported to the U.S. National HIV Surveillance System by December 2019 for persons ?13 years with HIV diagnosed during 2018, we described the time from HIV diagnosis to entry into the local surveillance system of key information. Timely reporting was defined as entry of cases ?30 days after diagnosis, and entry of sequence reports within 45 days of diagnosis.
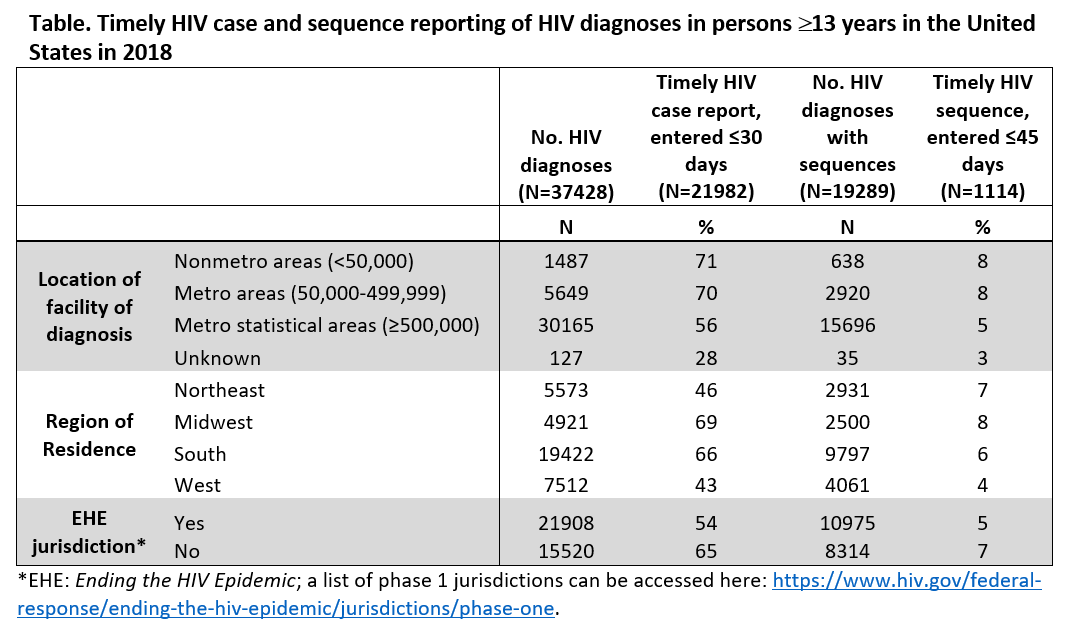
Among 37,428 HIV diagnoses in 2018, 21,982 (59%) were entered ?30 days after diagnosis. Median time to entry was 24 days (interquartile range [IQR]: 5.5–42.5) and varied by jurisdiction (range: 5–134). A higher proportion of HIV diagnoses met timely case reporting standards in: nonmetropolitan (71%) and small metropolitan areas (70%); the Midwest (69%) and South (66%); and jurisdictions not included in phase 1 EHE funding (65%) (Table). Of 19,289 HIV diagnoses with sequences reported, 71% had a sample collected within 30 days of diagnosis. However, only 6% had sequence data entered into the surveillance system within 45 days (median: 74 days; IQR: 31.5–117.5), with wide variation by jurisdiction (9.5–470). Time from diagnosis to specimen collection (median: 15 days; IQR: 0–30) was shorter than time from specimen collection to receipt and entry by the health department (median: 48 days; IQR: 27–70).
Over half of HIV diagnoses in 2018 were reported to the health department within one month, allowing analyses to detect clusters of increased diagnoses for further investigation. Reporting delays were greater for large metropolitan areas, the West, and the Northeast. Delayed availability of sequence results, which has implications for detecting molecular clusters, is driven by reporting rather than physician ordering of drug resistance testing, suggesting potential for improvement with changes in laboratory reporting and informatics practices. Additional EHE funding can be used to improve processes to expedite reporting and entry of case, laboratory, and key data into surveillance systems for real-time decision-making.