Patients with underlying medical conditions have a greater risk of developing severe COVID-19. Unlike vaccine-derived immunity which develops over time, administration of neutralizing monoclonal antibodies is an immediate, passive humoral immunotherapy, with the potential to reduce disease progression, emergency room visits, hospitalizations, and death.
In this phase 3 portion of the BLAZE-1 trial, a high-risk ambulatory cohort of 1035 patients with mild-to-moderate COVID-19 were randomly assigned 1:1 to receive a single intravenous infusion of a neutralizing monoclonal antibody combination treatment consisting of 2800mg bamlanivimab+2800mg etesevimab together, or placebo, within 3 days of laboratory diagnosis. The primary outcome was overall patient clinical status, measured by the proportion of patients who experienced COVID-19-related hospitalization or death by any cause by Day 29.
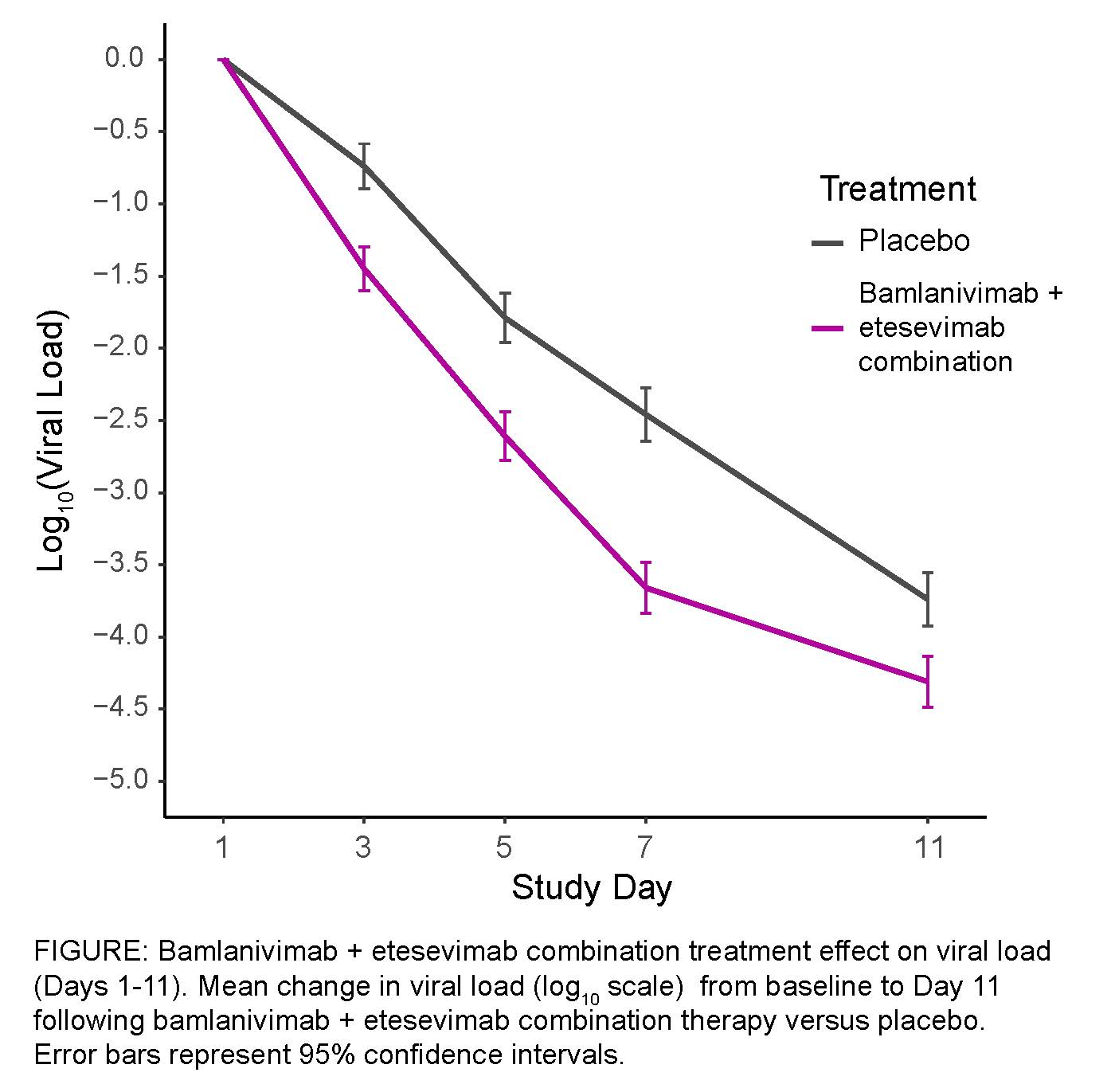
1035 patients were randomized and infused (mean age [SD]; 53.8 years [16.8], female (52%)). A 70% reduction in COVID-19-related hospitalization and death by any cause by Day 29 was observed in patients who received the bamlanivimab+etesevimab combination treatment (11/518 arm total) compared to those who received placebo (36/517 arm total) (?[95% CI]=-4.8[-7.4,-2.3])(p=0.0004). No deaths were observed among patients who received the combination treatment, 10 deaths were reported in the placebo group, at least 8 designated COVID-19-related. A significantly greater reduction in log10(viral load) from baseline at Day 7 was observed amongst patients who received bamlanivimab+etesevimab compared to placebo (?[95% CI]=-1.20[-1.46,-0.94])(p<0.00000001). The median time to sustained symptom resolution was shorter for those who received the combination treatment (days [95% CI]=8[7.0,8.0]) compared to those who received placebo (days [95% CI]=9[8.0,10.0])(p=0.007). Similar rates of adverse events were observed between placebo (60/517,11.6%) and combination treatment groups (69/518,13.3%).
2800mg bamlanivimab+2800mg etesevimab neutralizing monoclonal antibody combination therapy significantly reduced COVID-19-related hospitalizations and deaths amongst high-risk ambulatory patients and accelerated the decline in viral load and disease symptoms over time. This study confirms that early intervention with bamlanivimab + etesevimab greatly improves the clinical outcomes for high-risk ambulatory patients, and links reduction in nasopharyngeal viral load to clinically meaningful benefits.